
")

")

")
")


")
")




The right tools for calcium treatment.
We offer the most advanced and complete Modern PCI solutions
to master all types of coronary calcific lesions.
Optimal Therapies
Learn more about Calcified CAD and Optimal Therapies.
When it comes to identifying and treating calcific lesions, using the right tools makes all the difference. But many go-to strategies fall short, and can lead to compounding challenges.
Calcific Lesion Modification Strategy
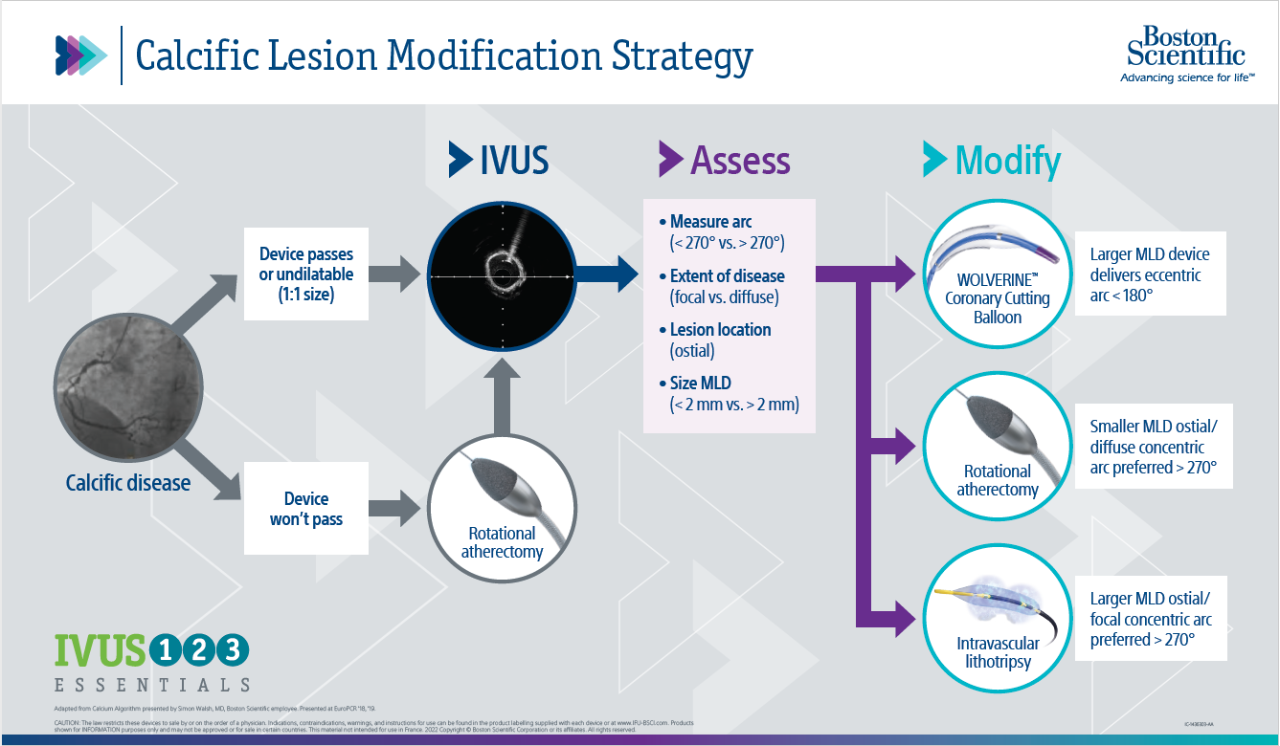
Optimal patient outcomes come from a systemic three-step approach to treat calcific lesions.
- See with IVUS
- Assess lesion length, plaque morphology and vessel size
- Prep the lesion, appropriately modify the calcium with cutting balloon (<180°), rotational atherectomy (>270°) or intravascular lithotripsy (>270°)
Diagnose with IVUS


IVUS is necessary for every procedure
- Allows for better treatment decisions

Prepare and Treat with the right tools for calcium
Identification is not the only area in which the status quo has failed to keep pace with your needs. POBA, a commonly used solution for addressing these lesions, can lead to dissections or perforations, leading to longer case time and limiting options for completing the case.
Rotational Atherectomy and Cutting Balloon treatment have proven efficacy for each level of calcification. Rotational Atherectomy is known to deliver exceptional outcomes, with multiple studies indicating that Rotational atherectomy results in high procedural success rates with acceptable short- and longer-term MACE rates considering the severity of patient and lesion characteristics.
In the recent DIRO study, a head to head comparison of orbital versus rotational atherectomy, rotational atherectomy (RA) demonstrated its superiority in treating calcified coronary lesions by achieving a larger maximum plaque modification area of 1.24 mm2 compared to orbital atherectomy at 0.89 mm2 (p<0.01)3. These findings prove the potential of RA for improved patient outcomes in managing calcified lesions.
To dive deeper into these insights, download our one-page overview of the DIRO study.
Cutting Balloon has proven successful in treating calcific lesions in the recent COPS study.
Calcium is being severely undertreated:



The COPS study, a prospective, multicenter, randomized controlled trial, has recently shed light on the efficacy and safety of using a cutting balloon (CB) for the treatment calcified lesions.
Three key takeaways from the COPS study are:
- Using a high-pressure CB results in a larger MSA (minimal stent area) and lower eccentricity of the stent at the level of the calcified segments compared to NCB (noncompliant balloon) angioplasty.5
- CB is safe compared to NCB angioplasty.5
- Using a CB instead of NCB optimizes lesion preparation in the case of significant calcifications (>270°).5
Interested in learning more?
The right tools for calcium
- Helps prevent complications and adverse events6


![]()
Education & Training with EDUCARE
When we challenge the status quo,
we advance patient outcomes.
Join our Complex PCI Community
Stay up-to-date via email on the latest advances in complex PCI

Request a Sales Rep
Fill out a quick form and one of our sales representatives will be in touch to answer any question you have.
Product catalogue
Download our product catalogue 2024 and stay up to date on our latest innovations.