
")

")

")
")


")
")



FFR guided PCI with new COMET™ FFR Pressure guidewire reveals the true picture

Key learnings
This case highlights:
- New Asahi co-developed COMET™ FFR Pressure guidewire’s ability to assess and perform PCI with multiple devices and reconnections

- How FFR guidance changes treatment strategy & alerts the operator to the need for further intervention in sub optimal PCI – where ischemia is still present
Patient History
- 70 year old man with previous PCI to RCA
- Baseline angiography showed diffuse disease and calcium of the mid LAD

Baseline angiography showed diffuse disease and calcium of the mid LAD
Watch the videoTechniques Used
- Pre dilation
- Stenting
- FFR pre and post treatment after each procedural step
COMET™ FFR Pressure Guidewire Characteristics
- Asahi co-developed for true workhorse capabilities
- Free rotation while steering and reliable re-connection
- Optical pressure sensor
- Easy to use IVUS / FFR multimodality interface
Clarify treatment strategy with FFR
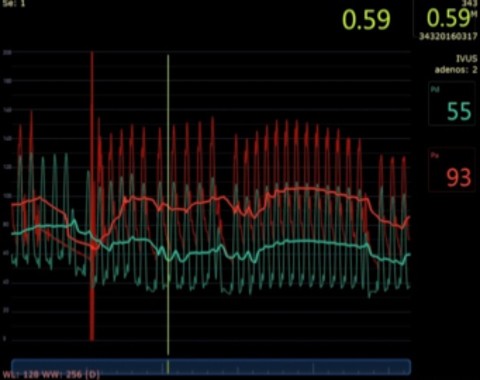
- FFR with the new COMETTM Pressure guidewire (0.14’’ Boston Scientific / Asahi Intecc) was selected to interrogate the lesion.
- COMET™ crossed the lesion easily and resting FFR showed a value of 0.76 (borderline value). Intracoronary adenosine was given and the value dropped to 0.59 (Figure 2)
Pre Dilatation Reveals Calcium
- The COMET™ Pressure guide wire was disconnected and the lesion was pre dilated with a 2.5 x 20mm EMERGE semi compliant balloon. Balloon inflation revealed significant calcium
- Due to significant calcium, the vessel was then treated with a non-compliant 2.5 x 15mm NC Quantum Apex. Next, the COMET™ pressure guidewire was re-connected and the resting Pd/Pa was 0.80. (not pictured)

Pre-dilation with semi compliant balloon
Watch the videoStents Placed
- Next, a Promus Premier 2.5 x38 DES was implanted (Figure 4) and inflated (Figure 5) and post dilated with a non-compliant balloon 2.5x20 mm

Positioning of Promus Premier 2.5 x 38 DES
Watch the video
Inflation of Promus Premier 2.5 x 38 DES
Watch the videoPost Stenting FFR performed, edge dissection discovered
- COMET™ was reconnected and IC adenosine was administered, giving an FFR value of 0.73. After further analysis an edge dissection was discovered at the distal stent edge.
- A Promus Premier 2.5 x 8mm DES was implanted to cover the distal edge dissection. After stent implantation and post dilation with NC Quantum Apex FFR showed yet another FFR value under 0.80.

Distal edge dissection and FFR value of 0.73
Watch the videoPost Stenting FFR performed, plaque shift discovered
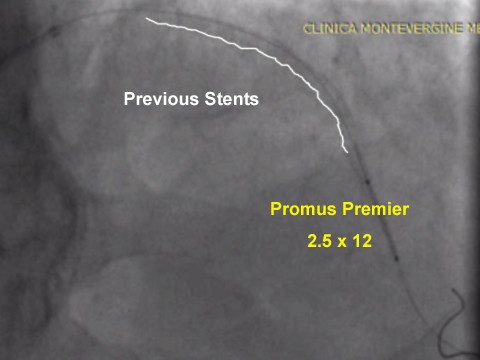
- Further analysis showed that the limited blood flow was caused by plaque shift due to the initial ballooning with long inflation times. To finish the case, the operator decided to implant the final 2.5 x12mm Promus Premier DES distal to the previous stents (Figure 7) with an FFR value of 0.84
Post Stenting FFR performed, non ischemic result

Final angio reading of distal left main
Watch the video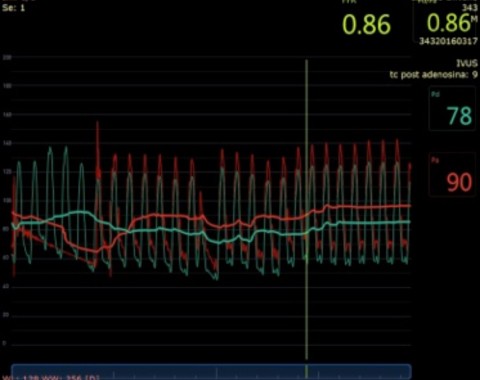
SUMMARY
- In this procedure, the use of FFR helped to clarify the continued presence of ischemia, requiring additional treatment methods.
- It’s important to note that the last FFR value was negative for ischemia, demonstrating the efficacy of FFR to guide the entire procedure, achieving an optimal final result.
- Numerous disconnections and reconnections of the new COMET™ FFR Pressure guidewire helped the operators to start, treat and perform final measurements without making the procedure longer and more expensive.
Join Our Complex PCI Community

Education & Training
Educare offers a comprehensive suite of education and training programs for Complex PCI.
Learn MoreResources
Download Case Study