
Personalized Physiological Insights
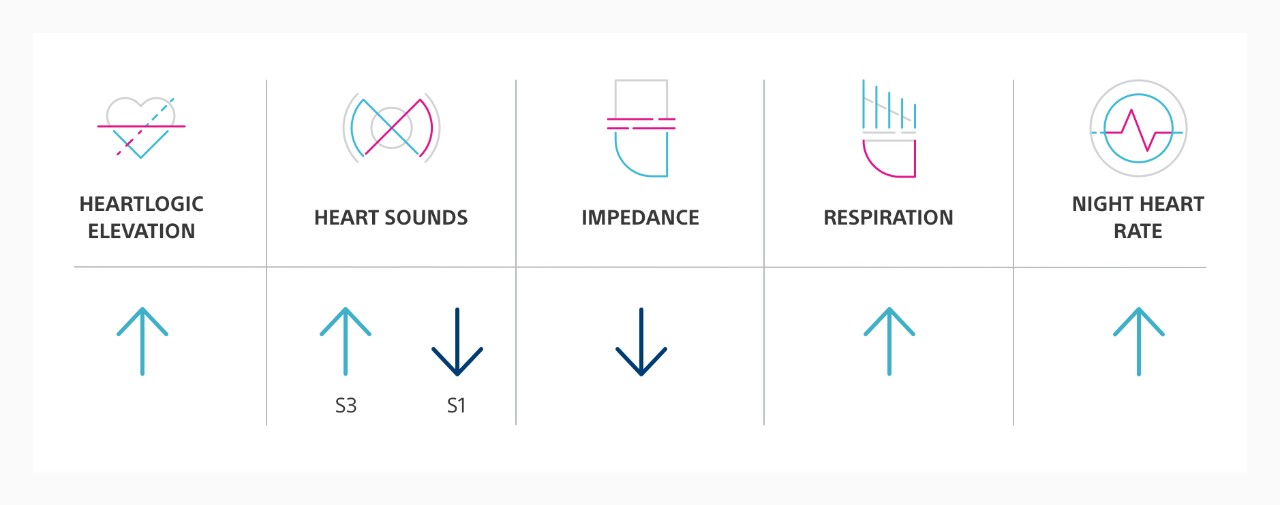
The HeartLogic Heart Failure Diagnostic uses automated intelligence to streamline your ability to see each patient’s physiologic response to arrhythmic and pacing changes.
HeartLogic and Atrial Fibrillation (AF) Events
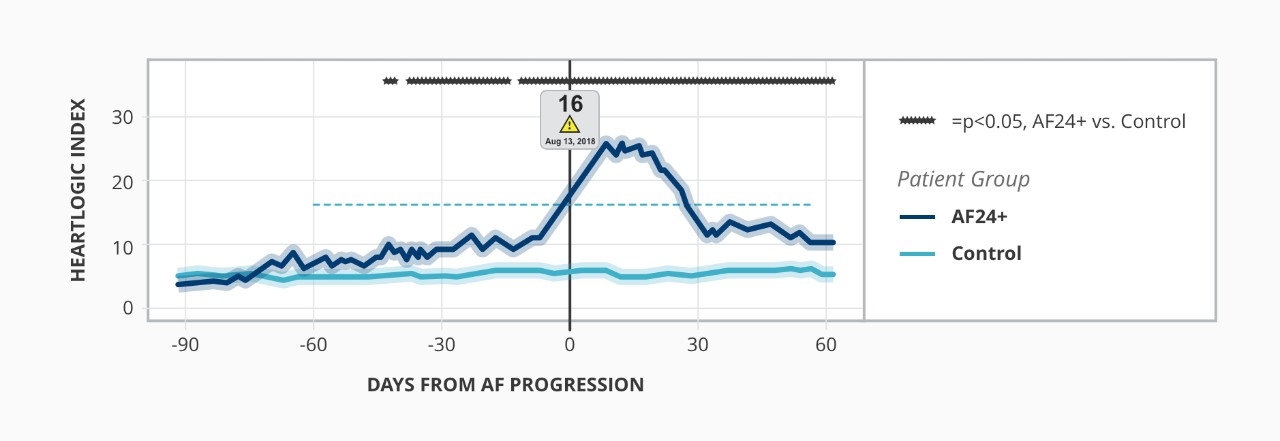
Heart Failure Progression Before and After AF
Relationship Between Atrial Fibrillation and HeartLogic Index1

Listen to HeartLogic experts discuss how they integrate heart failure care into daily EP practice.
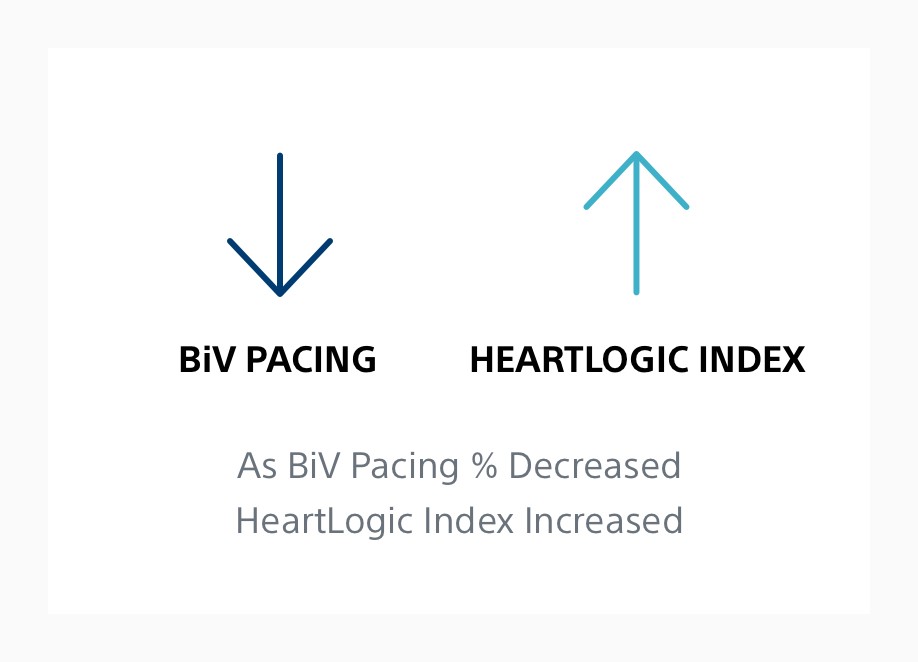
HeartLogic Sensors Reflect Sub-Optimal BiV Pacing % in CRT-D Patients2
- Minor sub-optimal BiV pacing percentages (~2%) were associated with progressively worse sensor and increasing HeartLogic index values.
- The proportion of days in HeartLogic alert was ~2X higher with <90% BiV pacing.
Read the abstract on page 370 for more information.
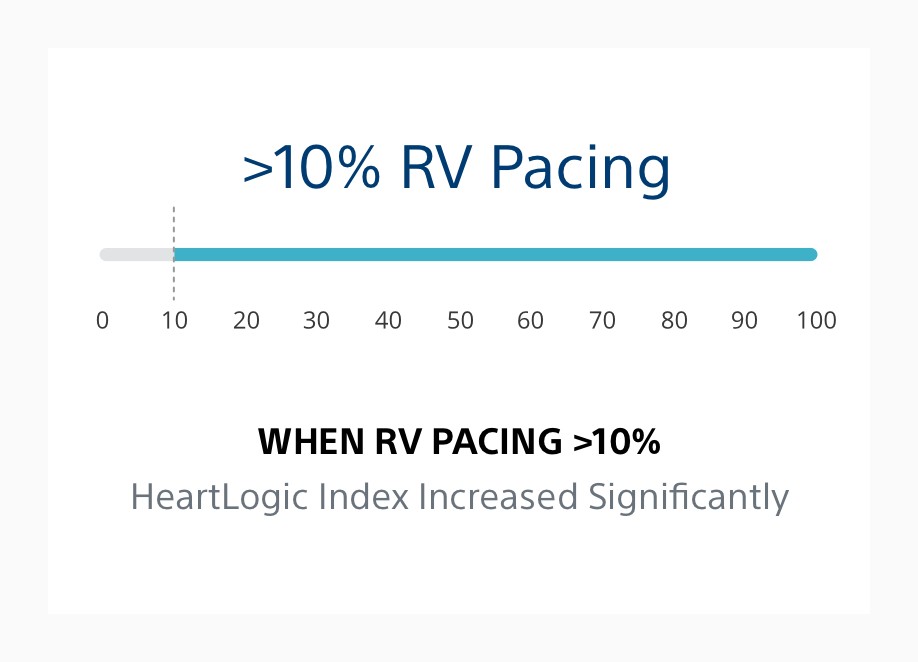
HeartLogic Sensors Reflect the Adverse Impact of RV Pacing in ICD Patients3
- Increased RV pacing percentage progressively worsened individual sensor values.
- HeartLogic index was significantly worse for RV Pacing >10%.
- HeartLogic may identify patients vulnerable to RV pacing.
Read the abstract on pages S58-S59 for more information.
Sign up for periodic emails and receive a HeartLogic fact sheet to share with your patients’ care teams.
Get results from this global trial evaluating the integration of HeartLogic into clinical practice.
Explore the data showing that HeartLogic provides a sensitive and timely predictor of impending HF events.4
LATITUDE NXT™ Remote Patient Management System: Indications, Safety and Warnings
References
1. Capucci A, Healey JS. Temporal association of atrial fibrillation with device-based heart failure status in patients with CRT. Oral presentation and LBCT presented at: EHRA Congress; March 2019, Lisbon, Portugal.
2. Varma N, Cao M, Schloss EJ, Ahmed R, Stolen C, Boehmer JP. Progressive worsening in device base failure sensors measurements are associated with sub-optimal BiV pacing percentages in CRT-D patients. J Heart Fail. 2019;21(Suppl. S1):370. doi: 10.1002/ejhf.1488.
3. Varma N, Stein KM, Thakur PH, Jones PW, Ahmed R, J Boehmer J. Multiparametric analysis of device based physiological sensors may identify ICD patients reacting adversely to right ventricular pacing [abstract]. Heart Rhythm. 2019;16(5):S58-S59.
4. Boehmer JP, Hariharan R, Devecchi FG, et al. A multisensor algorithm predicts heart failure events in patients with implanted devices: results from the MultiSENSE study. JACC Heart Fail. 2017 Mar;5(3):216-225. doi: 10.1016/j.jchf.2016.12.011