Kidney Resources
ICE Cryoablation Technology
Key Resources
Overview
Outcomes comparison
| Metric | How does cryo/ablation compare to partial nephrectomy (PN) | Limitations |
|---|---|---|
| Local recurrence free survival* | Level 1 data needed | Older data, meta-analyses include RF |
| Metastatic-free survival* | Ablation = PN | |
| Cancer-specific survival* | Ablation = PN | |
| Overall survival* | Level 1 data needed | Selection bias - ablation patients tend to be older with more comorbidities |
| Renal Function | Cryo/ablation > PN | |
| Safety | Cryo/ablation > PN | |
| Cost | Cryo/ablation > PN | |
| Quality of life | Cryo/ablation > PN |
*Oncological outcomes
Similar = | Better >
Case studies
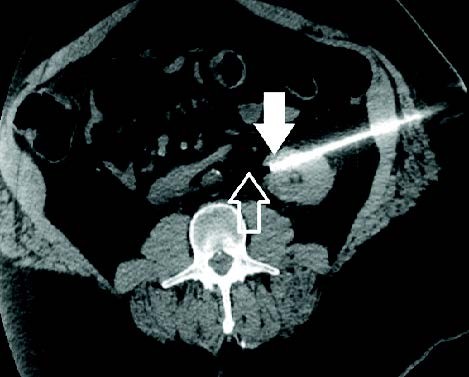
Adjacent Structures and RCC
A 66-year-old man presented with 2.0 cm x 2.1 cm left sided, endophytic RCC and biopsy confirmed clear cell renal cell carcinoma. Initial CR images on the day of the procedure demonstrated the lesion and adjacent colon, which would likely be injured if not moved. Cryoablation was performed with three IceRod™ 1.5 CX Needles for treatment and a yueh needle was utilized to introduce normal saline to hydrodissect away the adjacent colon. The patient had no pain or significant complaints; he was discharged and returned to work the same day of the procedure. He continues to be without evidence of residual/recurrent disease one-year later.
Shamar Young, MD I University of Minnesota I Minneapolis, MN
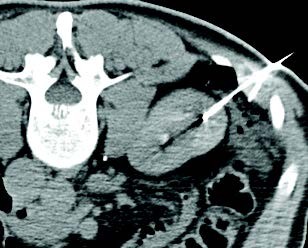
Using the Trajectory of the Needle to Protect Critical Structures
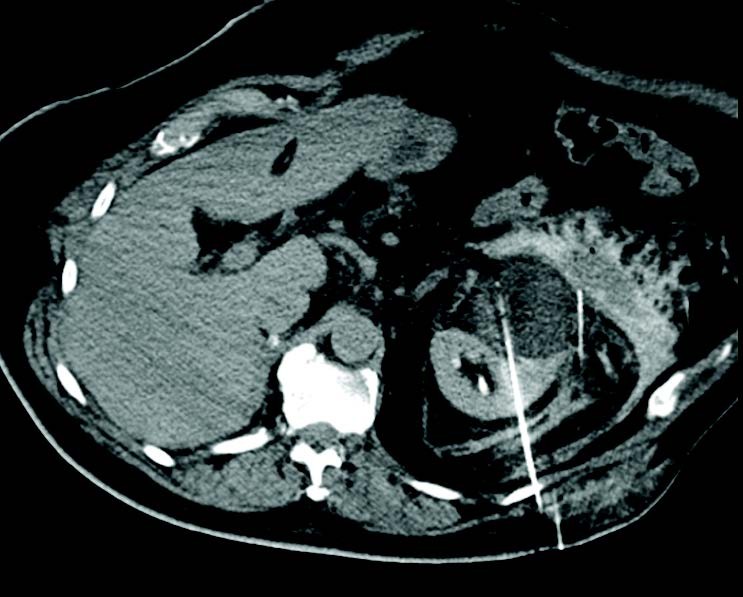
A 53-year-old man presented with 2.5 cm x 2.3 cm endophytic RCC in the anterior aspect of the lower pole of the left kidney. Cryoablation was performed with one IceForce™ 2.1 CX Needle. The tip of the needle was pointed toward the ureter since lethal ice only extends 5 mm beyond the tip of the needle. The patient was discharged the same day and follow-up imaging demonstrated no residual or recurrent disease 12-months post ablation.
AJ Gunn, MD I University of Alabama at Birmingham I Birmingham, AL
Cryoablation of 7 cm Renal Tumor after Previous Contralateral Nephrectomy
A 78-year-old man presented with right kidney multifocal RCC with vein invasion and concurrent 7 cm left anterior conventional clear cell RCC. The right tumor was treated with nephrectomy and the left tumor was treated with cryoablation 3 months after the nephrectomy. Hydrodissection was used to protect adjacent structures and 7 IceRod™ 1.5 PLUS needles were used to treat. There were no reported adverse events and early follow-up imaging of the left kidney confirmed adequate ablation.
Alex King, MD I University Hospital Southampton I Southampton, UK