TCT 2021 - Coronary Therapies
The Path to Modern PCI: Utilizing State-Of-The-Art Tools and Techniques to Optimize Patient Outcomes
Watch Dr. Ziad A. Ali, Dr. Kathleen Kearney and Dr. Simon J. Walsh discuss with Dr. J. Aaron Grantham their complex PCI approaches while leveraging SYNTAX II, IVUS utilization in Calcific lesions, and a live case walkthrough discussed throughout.
Additional details
The results from SYNTAX II prove that multivessel disease PCI patients can experience excellent, CABG-like outcomes out to five years. Despite case complexity, SYNTAX II, when compared to SYNTAX I PCI, shows statistically significant risk reduction in MACCE and ST due to the modern approaches such as –
- Imaging is key to Calcium detection, assessment, plan optimal treatment modalities and optimal stent placement
- Rotablation for the preparation of severely Calcified lesions is associated with a superior acute success rate compared to standard and modified balloons
- The Latest Generation DES plays an important role in elevating PCI Outcomes
OPTIMUM: Early Outcomes from a Prospective Registry of PCI in Patients at Prohibitive Risk for CABG
TCT Late-Breaking Clinical Science Session I, In Collaboration with Circulation
The outcomes of the OPTIMUM trial were presented during the TCT Late-Breaker Clinical Science Session by David E. Kandzari. This trial evaluated the outcomes of complex PCI patients who have multivessel or left main coronary artery disease and are deemed ineligible for CABG surgery. This session provides details of the OPTIMUM trial design and results of the study, including a panel discussion with commentary from Patrick W. Serruys, Jennifer Rymer, and David E. Kandzari.
Additional details
The OPTIMUM prospective registry comparing short-term mortality rates to predicted mortality.
21 U.S. Sites, N=750
Primary Endpoint: 30-day/in-hospital mortality in PCI cohort compared with predicted STS surgical risk
Clinical Outcomes
OPTIMUM's meaningful results inform decision making and outcomes for a high-risk and largely unstudied patient population relative to risk/benefit, procedural strategies, and completeness of revascularization with complex PCI.
Most complex trial to-date, evaluating a largely unstudied population:
70
Average Age
57%
Diabetic patients
38%
ACS patients
23%
Patients with heart failure
27%
Reporting no angina
32
Baseline SYNTAX Score
83%
Severe calcification
80%
Bifurcation
57%
CTO
79%
Long lesions (> 20mm)
Following complex PCI, short-term mortality rates are similar to predicted mortality using surgical risk models and considerably lower than the evaluating surgeon’s estimates.
- STS and EuroSCORE morality prediction models are intended to assess surgical mortality – these results are encouraging as they demonstrate similar PCI mortality rates
| Surgical Risk Prediction | 30-day / In-hospital Mortality (N=726) |
|---|---|
| STS Predicted Mortality* | 5.3 ± 5.7 |
| EuroSCORE II Predicted Mortality** | 5.7 ± 5.4 |
| Surgeon’s Predicted Mortality | 10.4 ± 12.3 |
| Observed 30-day / In-hospital Mortality | 5.6 |
6-month death: 12.3%
*STS Predicted Mortality score is a validated risk-prediction model for open surgery based on data from the STS National Adult Cardiac Surgery Database.
**EuroSCORE II Predicted Mortality score is a model used to estimate the in-hospital mortality after cardiac surgery provided by the European System for Cardiac Operative Risk Evaluation II.
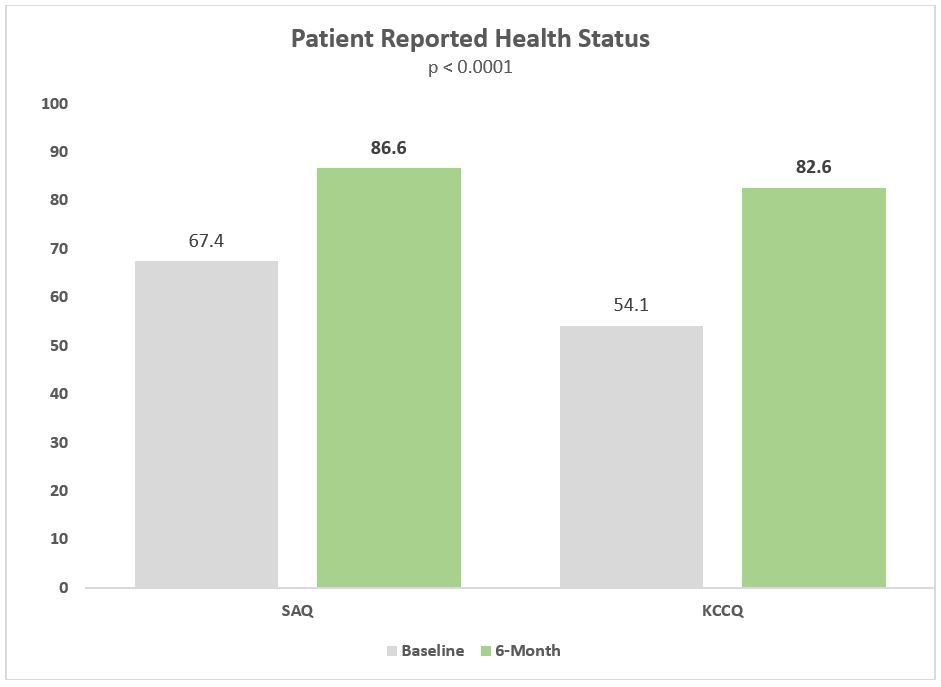
SAQ and KCCQ are both patient-reported health surveys assessing quality-of-life and angina frequency using a scale from 0-100, 1 being the lowest level of functioning
- SAQ: Seattle Angina Questionnaire
- KCCQ: Kansas City Cardiomyopathy Questionnaire
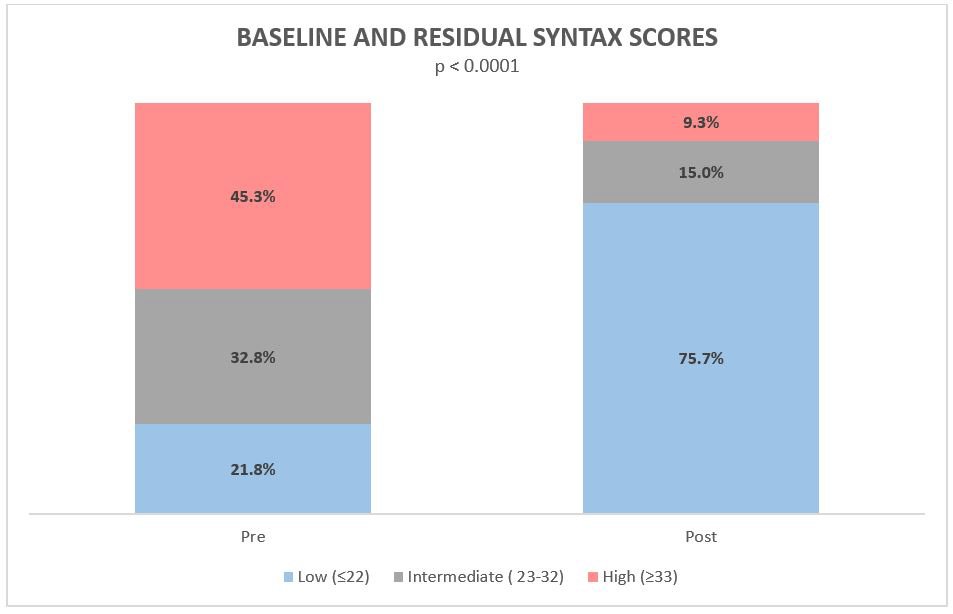
For patients which the heart team determined ineligible for coronary bypass surgery, PCI lowered residual Syntax Score from high to medium/low is 36% of patients.
| Baseline & Residual SYNTAX Scores | |
|---|---|
| Baseline (Pre-PCI) | 32.4 |
| Residual (Post-PCI) | 15.0 |
*The average baseline SYNTAX score in clinical trials is 24 – this is a very complex patient subset.
1 in 5
with left main and/or multivessel disease being deemed surgically ineligible
82%
of patients reporting no angina at 6 months
1/3
Patients achieved complete revascularization
64%
of cases utilized imaging