")

POLARIS
Multi-Modality Guidance System
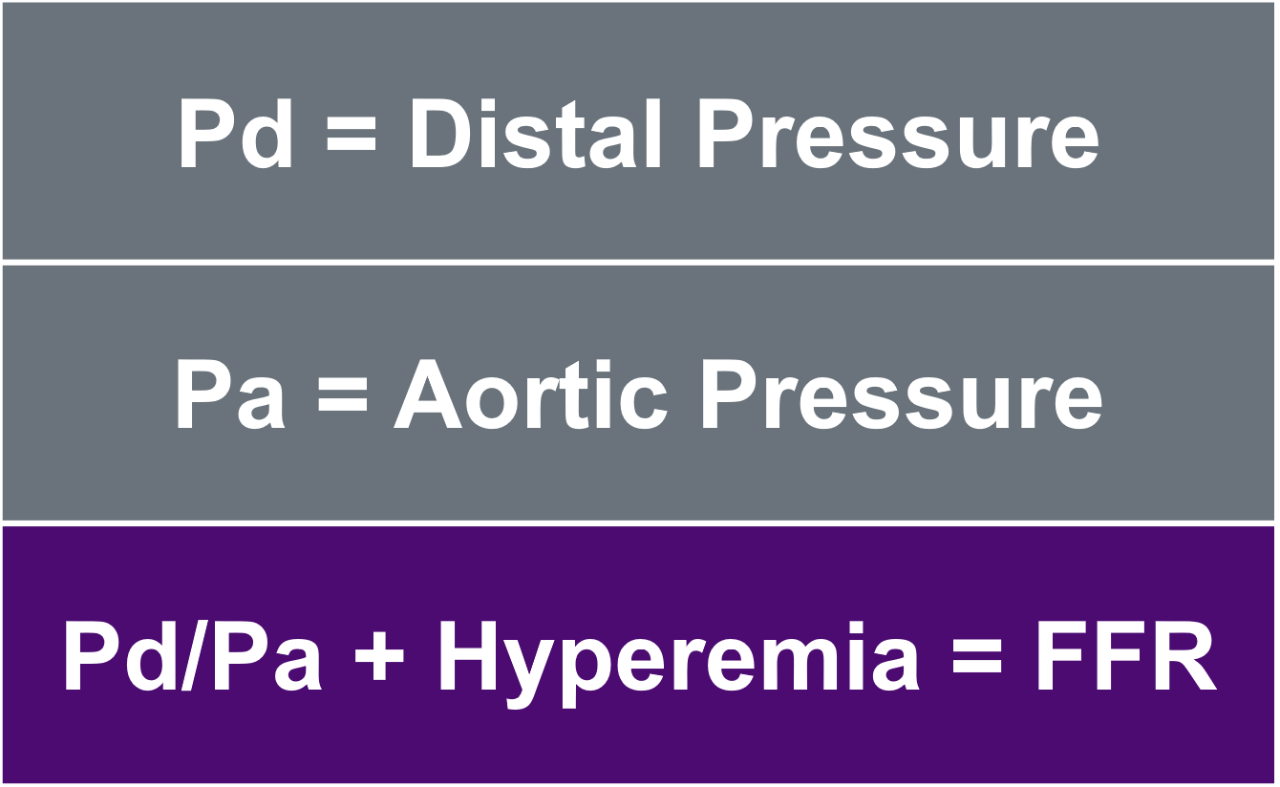
What is Fractional Flow Reserve (FFR)?

Key Resources

POLARIS Software – FFR Demo
View the unique features and intuitive workflow of our POLARIS FFR software, designed in partnership with clinicians.
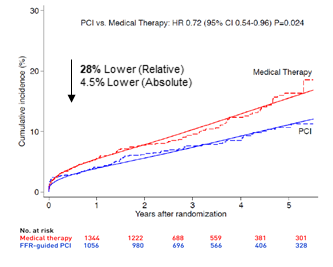
Hard Endpoints Favor FFR-Guided Strategy vs Medical Therapy Alone: A Pooled, Patient-Level Analysis of FAME II, DANAMI-3-PRIMULTI, and COMPARE-ACUTE1
Pooled analysis of 2,400 patients with stable CAD enrolled in FAME II, DANAMI-3-PRIMULTI & COMPARE-ACUTE were randomized to an FFR-guided strategy vs medical therapy alone. FFR-guided PCI resulted in a statistically significant reduction of cardiac death or MI at 5 years.
The relative risk reduction for cardiac death or MI was 28%. The absolute risk reduction for cardiac death or MI is 4.5%. FFR-guided PCI was also favored for all-cause death or MI. The combined endpoint was driven by
Cardiac Death or Myocardial Infarction