







")

Spermatic vein embolization in a grade II varicocele syndrome

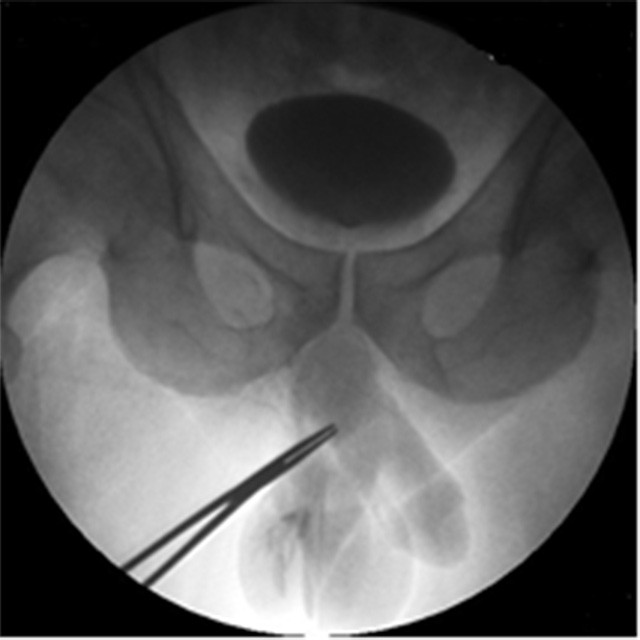
Diagnostic Angiography
A 47 year old patient was referred for treatment of bilateral varicocele.
A color-doppler-ultrasound examination detected, according to Sarteschi’s classification, a grade III-IV varicocele in the left-side and a grade I varicocele in the right-side.
We also detected qualitative and quantitative alterations of the spermiogram associated with clinical symptoms in the left scrotal side.
We decided to treat left varicocele with a right femoral approach.

First Treatment
The left spermatic vein was catheterized using a 5F (1.67mm) C3 cobra diagnostic catheter with an hydrophilic 0,035" guidewire.
We advanced the catether until its tip was in the inguinal canal so we made a Valsalva maneuver.
During temporary ligation of the scrotum with a snare, we administered 3 vials of 3% aethoxysclerol to obtain a complete embolization of the left pampiniform plexus. One month later, we observed a modest improvement in the spermiogram, but the doppler-ultrasound check showed an aggravation in the right varicocele from a grade I to a grade II.

Second Treatment
Result
In this patient the use of Direxion torquable microcatheter, with its pushability and trackability, for the treatment of right varicocele has proved to be crucial to the success of the procedure.
In fact, the small venous caliber and the fragility of the vessel associated with spasm determined by the passage of 0.035" (0.889mm) hydrophilic guidewire, would not have allowed the procedural success without the use of Direxion microcatheter.
Study and images courtesy of
Dr. Vincenzo Magnano San Lio – Chief of Radiology Department & Interventional Radiologist - "ARNAS Garibaldi Nesima" - Catania
Dr. Giuseppe Giordano – Dr. Stefania Bonomo – Dr. Claudia Trombatore - Interventional Radiologists - "ARNAS Garibaldi Nesima" - Catania